NEWS RELEASE August 2020
Mask Virus Removal Efficiency will be Important Focus in August 20 Webinar
There is growing evidence that N95 respirators will be the best mask selection for many applications and not just for doctors and nurses. A webinar on August 20 will provide debate and discussion on mask design as a function of viral load. The webinar will cover a number of factors related to the virus, the processes and applications, the mask designs and a common metric to measure all harm and good. Information on the market will be included as described at Click here to view a video description or Click here for the power point display.
One subject which needs attention and has not been previously analyzed is a new approach to measure mask efficiency based on one stop rather than direct. Now testing measures how much virus is initially captured on a mask but not how much is just stopping on its way to the final destination.
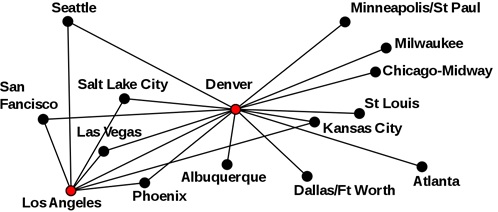
To measure the potential virus transmission of airline travelers from Seattle to Atlanta you need to take into account one stop as well as direct flights. The same is true for masks and filters.
How much virus is captured as larger droplets on the filter media and then converted to small aerosols? Research is now showing that with inefficient masks and filters the one stop flight is a significant contributor.
Experts on droplet evaporation have much to add to this discussion. We conducted an interview with one of these experts July 24, 2020 - Abhishek Saha Interview on Droplet Travel https://youtu.be/F790vEfB4ws
In our Alert on August 11 we quoted Duke University Researchers who said, "We were extremely surprised to find that the number of particles measured with the fleece actually exceeded the number of particles measured without wearing any mask."
On August 6 we quoted the Center on Infectious Research “We do, however, have data from laboratory studies that indicate cloth masks or face coverings offer very low filter collection efficiency for the smaller inhalable particles we believe are largely responsible for transmission.”
If a mask stops the larger droplet but is not able to capture smaller aerosols then it stands to reason that as the droplet evaporates and water vapor, smaller droplets, and salts make their way through the mask they will carry a significant amount of the virus from the larger droplet.
These questions can be laid to rest with one stop testing. Instead of just injecting droplets into a mask and measuring the initial capture over a few seconds, it will be necessary to measure the emission from the mask over time. A person may wear a mask for several hours and will be exhaling breath as many as 1000 times during that period. So this whole procedure can be duplicated in a laboratory setting.
The average individual in a room of average air purity will breath in and exhale many millions of particles every minute. Here are the particles by size in each breath.
During the two hour period after a large droplet is deposited on the mask interior the wearer will exhale some percentage of more than 700 million particles 0.1 micron and larger (depends on mask efficiency). How will these particles interact with the large droplet? How many will act as carriers for virus?
We need input on this from filter companies and in the Alert on August 12 display some slides prepared by Kari Luukkonen of Fibertex relative to the number of particles in filter intake air in various locations and also the impact of humidity, fog etc.
One challenge will be to measure small droplets which flow through openings around the mask as well as those which flow through the mask. This being the case the difference between respirators and surgical masks needs to be understood.
Another variable is the amount of virus which will cause infection and the difference between momentary and continuous transmission. The only rationale for cloth surgical masks is that they prevent a momentary barrage of millions of viral particles. But what if those particles are transmitted as small aerosols over time. If the recipient receives those millions of particles over two hours is that the same as if he received them in 5 seconds.
A related issue is what is the minimum infectious dose. If it is millions of particles a surgical mask makes some sense. But if it is thousands then the aerosol re-emission is important. Also a large droplet will lodge in nasal passages whereas small aerosols will reach the lungs. What are the health implications?
The August 12 Alert quotes UK experts who say the minimum infectious dose is 100 to 1000 and that accumulation over time is significant.
For more information on the webinar or to register click on http://home.mcilvainecompany.com/index.php/2-uncategorised/1574-coronavirus-webinars